

Race Correction in Kidney Function Algorithms and Disparities in Kidney Transplant Wait List Time
Race Correction in Kidney Function Algorithms and Disparities in Kidney Transplant Wait List Time
Bias in Healthcare Algorithms

It is National Kidney Month! During graduate school, I worked in Transplant Medicine at Medstar Georgetown Transplant Institute. Since I was studying epidemiology and data science, I searched for ways to combine my interests. Eventually, I stumbled into learning about Bias in Healthcare Algorithms. I plan to explore algorithmic bias in public health more in the newsletter. Stay tuned!
Eliminating the CKD-EPI equations race coefficient from kidney transplant eligibility criteria could reduce transplant wait times for African Americans thus reducing the disparity in time to transplant. Overall, African Americans who have higher rates of diabetes and hypertension are more likely to not get listed for a transplant compared to other groups and have longer wait times. (Schold et al.) Some argue that the race correction in the CKD-EPI equations estimation of glomerular filtration rate(eGFR) plays a role in this. Researchers argue that removing race from the biased algorithm for GFR estimation could help reduce the time to transplant.
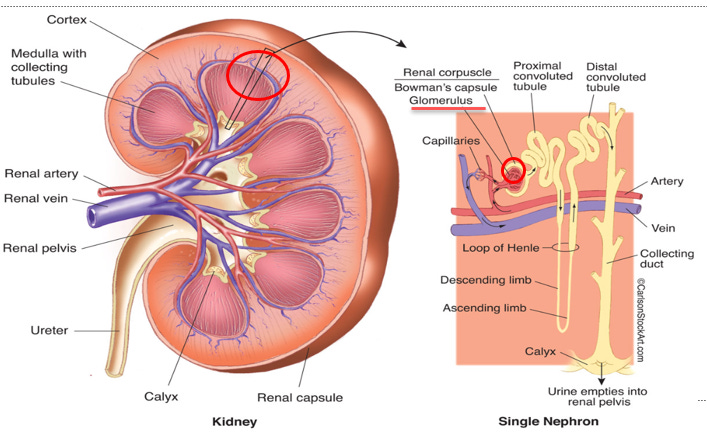
The eGFR is a surrogate marker for the number of functioning nephrons in a kidney. See the figure above to see a nephron. The nephrons are made of glomeruli and tubules. The glomerulus filters waste out of blood and the waste is carried away by the tubules. eGFR is used because getting a precise measure of glomerular filtration rate (GFR) involves using filtration markers such as inulin, iothalamate, or iohexol is more complicated and invasive.(Stevens et al.) There are three equations to estimate GFR the Cockcroft-Gault, MDRD equation, and the CKD-EPI equation. (Levey et al. “Gfr Estimation: From Physiology to Public Health”) The CKD-EPI equation is used the most often, so we will discuss this algorithm.
The normal GFR for a kidney is 120 to 130 ml/min/1.73m2.(Levey et al. “Gfr Estimation: From Physiology to Public Health”) At this GFR, the kidneys are functioning efficiently, and they are filtering out excess waste and fluid. In the hospital setting, GFR is used to understand patients’ symptoms, abnormal labs, adjust drug doses, and assess the risk of kidney disease. (Levey et al. “A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Modification of Diet in Renal Disease Study Group”)

When an individual’s GFR starts to decline, they will likely progress through the five stages of kidney disease as seen above. The early stages of kidney disease may include a decline in GFR, but the patients are asymptomatic, from Stage 1 to Stage 2. Kidney disease is considered chronic when the GFR is below 60 ml/min/1.73m2 for three or more months. (Levey et al. “Gfr Estimation: From Physiology to Public Health”) This would be Stage 3a. As kidney function worsens, the patient will progress to Stages 3b and 4. When the kidney is no longer filtering waste out of the kidney, the patient will progress to end-stage renal disease, Stage 5. At stage 5, patients may be referred to dialysis or receive an organ transplant with a living or deceased donor. (Abecassis et al.) At stage 5, the patient will die without getting a kidney transplant. At each stage, GFR plays a role in assessing the patient’s risk of kidney failure.
When a transplant is considered an option for someone with Chronic Kidney Disease (CKD), they will go through some or all of the following steps. First, a patient’s nephrologist will determine if a patient is suitable to be referred to a transplant center. GFR is one of the considerations used. If they are suitable and want a transplant, they are referred to a transplant center. When a patient is evaluated for transplant, a medical review board at a transplant center decides whether the patient is suitable for transplant. (Arriola) The medical review board will review labs and major organ systems to see if they are any conditions that would make the transplant less likely to succeed. If they are found healthy enough for transplant and have financial and social support, the patient is added to the national transplant waitlist at United Network for Organ Sharing (UNOS). (Levin et al.) The CKD-EPI algorithm, which estimates GFR, is one of the components of this process. At this point, the patient could have a living donor or deceased donor transplant, which is partially determined by their GFR.
eGFR plays a role in the kidney allocation system. Under the current system of kidney allocation, kidney transplant candidates are not registered on the wait list until their globular filtration rate is decreased to 20 ml/min per 1.73 m2 or less per UNOS requirements. (Stevens et al.) For those who need a transplant, the waiting time is calculated using 3 criteria. 1. When the candidate starts dialysis 2. The eGFR is below 20 ML/min/1.73m2 and 3. the date the eGFR is less than 20 ml/min/1.73m2 and if they were registered before starting dialysis. (Procurement)
When looking at the supply of kidneys for this eligible for transplant, the demand for kidneys is far greater than the supply. In 2017, 30,918 candidates were added to the waiting list. (Hart et al.) However, only 20000 kidneys transplants were performed in 2017. Many patients wait for a kidney transplant and never receive one and eGFR plays a role in this. In 2007, 12 percent of waitlisted kidney transplant candidates were waiting 5 or more years versus 15 percent in 2017. There are trends that show that wait times are increasing for kidney transplants. (Hart et al.)
There are health disparities on the kidney transplant waitlist. The disparities start with gaining access to the wait list There are disparities on when patients get referred to a nephrologist which is required to get on the transplant list. A late referral is associated with the less likelihood of getting a transplant.(Cass et al.) Those with a low socioeconomic status and African Americans tend to have longer waitlist times and it takes longer for them to get referred to transplant. Low educational attainment is associated with a longer time and more difficulty in getting on the transplant waitlist. Non-English speakers, women, type of dialysis center, those with diabetes, and obesity typically have longer wait list times. (Schold et al.) (Navaneethan and Singh)
However, just because someone is listed for transplant does not mean they will stay on this transplant waitlist, they can become inactive on the waitlist. In the United States, 33891 were removed from the waitlist in 2017. (Hart et al.) There are many reasons candidates can become inactive or removed on the waitlist. The most common are that they have an incomplete workup, insurance issues, too ill, too healthy, they want a living donor transplant, or the asked to be removed. About 25% of candidates listed as inactive never become active again or die on the waiting list. (Delmonico and McBride) About 5% of those on the wait list die every year and 7 % of diabetics on the wait list end up dying. Also, the mortality rate increases with age of the person on the waitlist. 33% of candidates on the wait list are African American. (System)
However, if candidates are referred early for kidney transplant, the mortality rates could drop. (Ku et al.) The eGFR plays a role in a nephrologist deciding whether to refer a patient for transplant. However once referred and listed, there are disparities in getting off of the kidney transplant waitlist. While African Americans are overrepresented with end stage renal disease, they are disparities when receiving kidney transplants. Caucasians are more likely to receive living donor kidney transplants, which typically have a better survival and less complications. (Schold et al.) African Americans are more likely to have a deceased donor transplant or a transplant from cardiac death donors which is associated with worse post-transplant outcomes. (Taber et al.)

The eGFR which kidney transplant referral decisions are based on is calculated from the CKD-EPI equation, the most used kidney function algorithm. The CKD-EPI equation is used because it is invasive and time intensive to measure GFR directly. There is a race correction coefficient in the CKD-EPI equation increases eGFR in African Americans patients by 16%. The race coefficient in the CKD-EPI equation is based on studies that were it was not clear how African American race was determined. (Braun et al.) Also, there are no biological differences between African Americans and whites, so it there is not a strong scientific basis to use the race coefficient in the CKD-EPI equation. Also, CKD-EPI equation does not consider racial differences due to structural racism in the United States. (Ahmed et al.) This is likely leading to disparities in kidney transplantation. (Eneanya et al. “Race-Free Biomarkers to Quantify Kidney Function: Health Equity Lessons Learned from Population-Based Research”)
Some researchers think the eGFR score being used so heavily reduces fairness. Medications like antibiotics can be withheld based on the eGFR score. The eGFR score helps determination of CKD diagnosis and stage. (Norris et al.) Also, some groups like African Americans are often not be referred to potentially helpful clinical trials because of their eGFR score. (Eneanya et al. “Reconsidering the Consequences of Using Race to Estimate Kidney Function”) The risk of increased time on the kidney transplant waitlist also depends on a reliable measure of eGFR. For African Americans and Caucasians, their eGFR score could make a difference in whether the candidate receives an organ in early enough to increase their chances of survival.
However, some researchers believe that eliminating the African American coefficient for eGFR will lead to unintended consequences. For example, it could lead to early transplant, getting dialysis too early, CKD getting over-diagnosed, underdosing, decrease access to testing, and less access to treatments based on Levey et al. The study pooled data from ten studies to compare the CKD-EPI equation with and without the race coefficient for African Americans. (Levey et al. “Estimation of Glomerular Filtration Rate with Vs without Including Patient Race”) Some studies suggest the prevalence of CKD in African Americans would increase.
There have been studies performed that searched for ways to stop using the race-corrected GFR. One study found that removing the race coefficient from the eGFR calculation increased the eligibility of African Americans for transplant. Also, it would get African Americans referred to a nephrologist sooner which could help them get on the waitlist sooner. Also, it would reclassify those with chronic kidney disease at a 3b, 4, or higher stage which could help them get on the waitlist or transplanted sooner. (Diao et al.) One study found that nearly a third of African Americans would be reclassified to a more severe stage if the race correction coefficient was removed from the equation. The downside of not using the race correction algorithm is that a small group of people will lose medication access. (Norris et al.)
There are health disparities in time to kidney transplant partially due to the race-corrected eGFR. While some healthcare systems have begun to eliminate the use of the race-corrected eGFR, more work is needed to increase the adoption of removing the race coefficient or another measure of kidney function. For the future, there should be a routine audit of kidney transplant algorithms to make sure more bias is not introduced into the patient care. This suggestion has been discussed in the literature, and it is important moving forward. (Eaneff et al.; Norris et al.)
References
Abecassis, M. et al. “Kidney Transplantation as Primary Therapy for End-Stage Renal Disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (Nkf/Kdoqitm) Conference.” Clin J Am Soc Nephrol, vol. 3, no. 2, 2008, pp. 471–80, doi:10.2215/CJN.05021107.
Ahmed, S. et al. “Examining the Potential Impact of Race Multiplier Utilization in Estimated Glomerular Filtration Rate Calculation on African-American Care Outcomes.” J Gen Intern Med, vol. 36, no. 2, 2021, pp. 464–71, doi:10.1007/s11606–020–06280–5.
— -. “Associations between Web-Based Resource Use and Patient Centered Outcomes in Chronic Kidney Disease (Ckd).” American Journal of Kidney Diseases, vol. 73 (5), 2019, p. 647.
Arriola, K. J. “Race, Racism, and Access to Renal Transplantation among African Americans.” J Health Care Poor Underserved, vol. 28, no. 1, 2017, pp. 30–45, doi:10.1353/hpu.2017.0005.
Balch, Bridget. “Confronting Race in Diagnosis: Medical Students Call for Reexamining How Kidney Function Is Estimated.” vol. 2021, AAMC, 2020.
Bragg-Gresham, J. et al. “Prevalence of Chronic Kidney Disease among Black Individuals in the Us after Removal of the Black Race Coefficient from a Glomerular Filtration Rate Estimating Equation.” JAMA Netw Open, vol. 4, no. 1, 2021, p. e2035636, doi:10.1001/jamanetworkopen.2020.35636.
Cass, A. et al. “Late Referral to a Nephrologist Reduces Access to Renal Transplantation.” Am J Kidney Dis, vol. 42, no. 5, 2003, pp. 1043–9, doi:10.1016/j.ajkd.2003.07.006.
Delmonico, F. L. and M. A. McBride. “Analysis of the Wait List and Deaths among Candidates Waiting for a Kidney Transplant.” Transplantation, vol. 86, no. 12, 2008, pp. 1678–83, doi:10.1097/TP.0b013e31818fe694.
Diao, J. A. et al. “Clinical Implications of Removing Race from Estimates of Kidney Function.” JAMA, vol. 325, no. 2, 2021, pp. 184–86, doi:10.1001/jama.2020.22124.
Eaneff, Stephanie et al. “The Case for Algorithmic Stewardship for Artificial Intelligence and Machine Learning Technologies.” Jama, vol. 324, no. 14, 2020, pp. 1397–98.
Eneanya, N. D. et al. “Race-Free Biomarkers to Quantify Kidney Function: Health Equity Lessons Learned from Population-Based Research.” Am J Kidney Dis, 2021, doi:10.1053/j.ajkd.2020.12.001.
— -. “Reconsidering the Consequences of Using Race to Estimate Kidney Function.” JAMA, vol. 322, no. 2, 2019, pp. 113–14, doi:10.1001/jama.2019.5774.
Hart, A et al. “Optn/Srtr 2017 Annual Data Report: Kidney.” American Journal of Transplantation, vol. 19, 2019, pp. 19–123.
Inker, L. A. et al. “A New Panel-Estimated Gfr, Including Β.” Am J Kidney Dis, vol. 77, no. 5, 2021, pp. 673–83.e1, doi:10.1053/j.ajkd.2020.11.005.
Ku, E. et al. “Racial Disparities in Eligibility for Preemptive Waitlisting for Kidney Transplantation and Modification of Egfr Thresholds to Equalize Waitlist Time.” J Am Soc Nephrol, vol. 32, no. 3, 2021, pp. 677–85, doi:10.1681/ASN.2020081144.
Levey, A. S. et al. “Gfr Estimation: From Physiology to Public Health.” Am J Kidney Dis, vol. 63, no. 5, 2014, pp. 820–34, doi:10.1053/j.ajkd.2013.12.006.
— -. “Estimation of Glomerular Filtration Rate with Vs without Including Patient Race.” JAMA Intern Med, vol. 180, no. 5, 2020, pp. 793–95, doi:10.1001/jamainternmed.2020.0045.
Levin, Adeera et al. “Kidney Disease: Improving Global Outcomes (Kdigo) Ckd Work Group. Kdigo 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.” Kidney international supplements, vol. 3, no. 1, 2013, pp. 1–150.
Navaneethan, S. D. and S. Singh. “A Systematic Review of Barriers in Access to Renal Transplantation among African Americans in the United States.” Clin Transplant, vol. 20, no. 6, 2006, pp. 769–75, doi:10.1111/j.1399–0012.2006.00568.x.
Norris, Keith C et al. “Removal of Race from Estimates of Kidney Function: First, Do No Harm.” Jama, vol. 325, no. 2, 2021, pp. 135–37.
Procurement, Organ. “Organ Procurement and Transplantation Network.” HRSA, DHHS, vol. 9, 2016.
Schold, J. D. et al. “Barriers to Evaluation and Wait Listing for Kidney Transplantation.” Clin J Am Soc Nephrol, vol. 6, no. 7, 2011, pp. 1760–7, doi:10.2215/CJN.08620910.
Stevens, L. A. et al. “Assessing Kidney Function — Measured and Estimated Glomerular Filtration Rate.” N Engl J Med, vol. 354, no. 23, 2006, pp. 2473–83, doi:10.1056/NEJMra054415.
System, United States Renal Data. “2020 Usrds Annual Data Report: Epidemiology of Kidney Disease in the United States.”, 2020.
Vyas, Darshali A et al. “Hidden in Plain Sight — Reconsidering the Use of Race Correction in Clinical Algorithms.” Mass Medical Soc, 2020.